
A range of oral surgery procedures are offered at High Street Dental Practice by specialist oral surgeon Prem Nair. These include:
- Simple and complex dental extractions
- Removal of simple and complex wisdom teeth
- Removal of retained roots
- Orthodontic extractions
- Exposure and bonding of unerupted teeth for orthodontics
- Simple and complex dental implants
- Surgical management of failed endodontic treatment (Apicectomy)
- Cyst enucleation associated with teeth
- Pre-prosthetic surgery
- Labial and lingual frenectomies
- Bone grafting and sinus lifts
Management of Wisdom teeth
Wisdom teeth are normally the last molar teeth on the upper and lower jaw to erupt. They normally erupt when you are 18-24 but there are lots of incidences when they erupt earlier or much later. Impacted wisdom teeth are those, which cannot erupt into the mouth, mostly because they are impacted against the adjacent teeth or the bone.
The gum tissue partially covering the wisdom teeth will lodge food debris and cause inflammation of the tissues around as well as infection. This is mostly seen with the lower wisdom teeth and could be an extremely painful condition. Fully erupted wisdom teeth seldom cause problems. An experienced dentist or a Specialist Oral surgeon should treat symptomatic complicated wisdom teeth.
Ref: www.nice.org.uk
Management of retained roots
Symptomatic roots are usually best removed under local anaesthetic by a Competent Practitioner.
It is recommended to limit operating time to less than 45 minutes and to have adequate pre-operative X-rays. Complex retained roots may be referred to a specialist Oral surgery service.
Asymptomatic roots, which are not communicating with the mouth and have no evidence of infection radiologically and clinically, may be left alone. These buried roots should be reviewed periodically by clinical examination and if indicated supporting X-rays.
There are a few clinical indications for the removal of asymptomatic tooth roots and these include roots in the region of planned Implant or bridge and denture construction. However, there can be complications from the removal of tooth roots which can lead to significant loss of supporting bone, damage to adjacent teeth and roots and damage to nearby nerves.
The benefit of removing the roots must outweigh the risks.
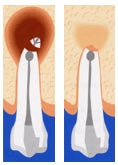
Surgical Endodontics (Apicectomy)
Teeth that have failed following root canal treatment (endodontics) are salvaged by surgical endodontics (Apicectomy). The aim of this treatment is to remove the infected tissue from the root tip and seal this area by a non-tissue irritating restoration. This treatment is more successful in single-rooted teeth (upper and lower anterior teeth). However, the failure rates go up with multirooted teeth.
There is strong evidence to show that periapical pathology is best treated endodontically even if a crown or a bridge is in place.
Symptomatic persistent periapical pathology is best managed by repeat endodontic therapy and if necessary by a specialist endodontist.
Essentials before Considering Surgical Endodontics
- Sound periodontal status and good Oral hygiene
- Good bone support for the tooth
- Adequate root filling with adequate apical seal and if necessary repeat root filling
- Sound coronal seal by either a restoration or crown
Indications
- Persistent signs and symptoms after repeated, quality good endodontics (Root canal treatment)
- Enlarging and persisting cystic lesions on repeat X-rays.
- Endodontics not possible because of sclerosed canals or broken instruments
- Lateral perforation in an accessible site.
Referral for Apical Surgery
Only patients meeting the above criteria should be considered for apical surgery referral.
Ref: RCS of England Web site and the FDS site

Management of Labial and Lingual Frenum
Labial Frenum is the thick fibrous attachment normally in the middle of the upper and lower lip. It causes spacing between the upper central incisors. Surgical treatment is often recommended.
Lingual Frenum is a thick fibrous attachment under the tongue, which restricts tongue movement.
Frenum of the upper and lower lips can, on occasion, affect the gingival attachment around incisor teeth leading to a loss of attachment and periodontal problems. Median diastema (space) between the central incisor teeth may be caused by the thick fleshy upper labial Frenum.
The lingual Frenum may restrict tongue movement (ankyloglossia) and also affect the gingival attachment. It may also affect suckling in infants and very rarely speech/ phonation (tongue tip sounds).
Management of Labial Frenum with or Without Diastema
Frenectomy is not usually considered until the canine teeth have erupted and orthodontic treatment planned. It is therefore unusual for a patient to be considered for Frenectomy less than ten years old. Labial Frenectomy can usually be performed under local anaesthesia by a competent practitioner with a cooperative child.
Management of Lingual Frenum
NICE has issued guidance where only babies whose tongue-tie interferes with breastfeeding should be offered a release procedure. This can be performed on many newborns in the outpatient departments without any anaesthetic (Local or General).
Lingual Frenectomy may be considered in children over 1 year of age if there are significant problems of ankyloglossia and a traumatic gingival attachment exists. There is little evidence (from Speech and Language therapists) that releasing tongue-tie improves a child’s speech development. The release of the tongue-tie can be performed under general anaesthetic in young children as a day case or under local anesthesia when age allows.
Ref: www.nice.org.uk